There's a pattern we keep seeing across sites, and it's costing more patients than most coordinators realize.
A patient picks up the phone after seeing a trial ad. They spend 30 minutes on the line answering eligibility questions with your recruiter. They're engaged. They're motivated. They think they're moving forward.
Then they wait.
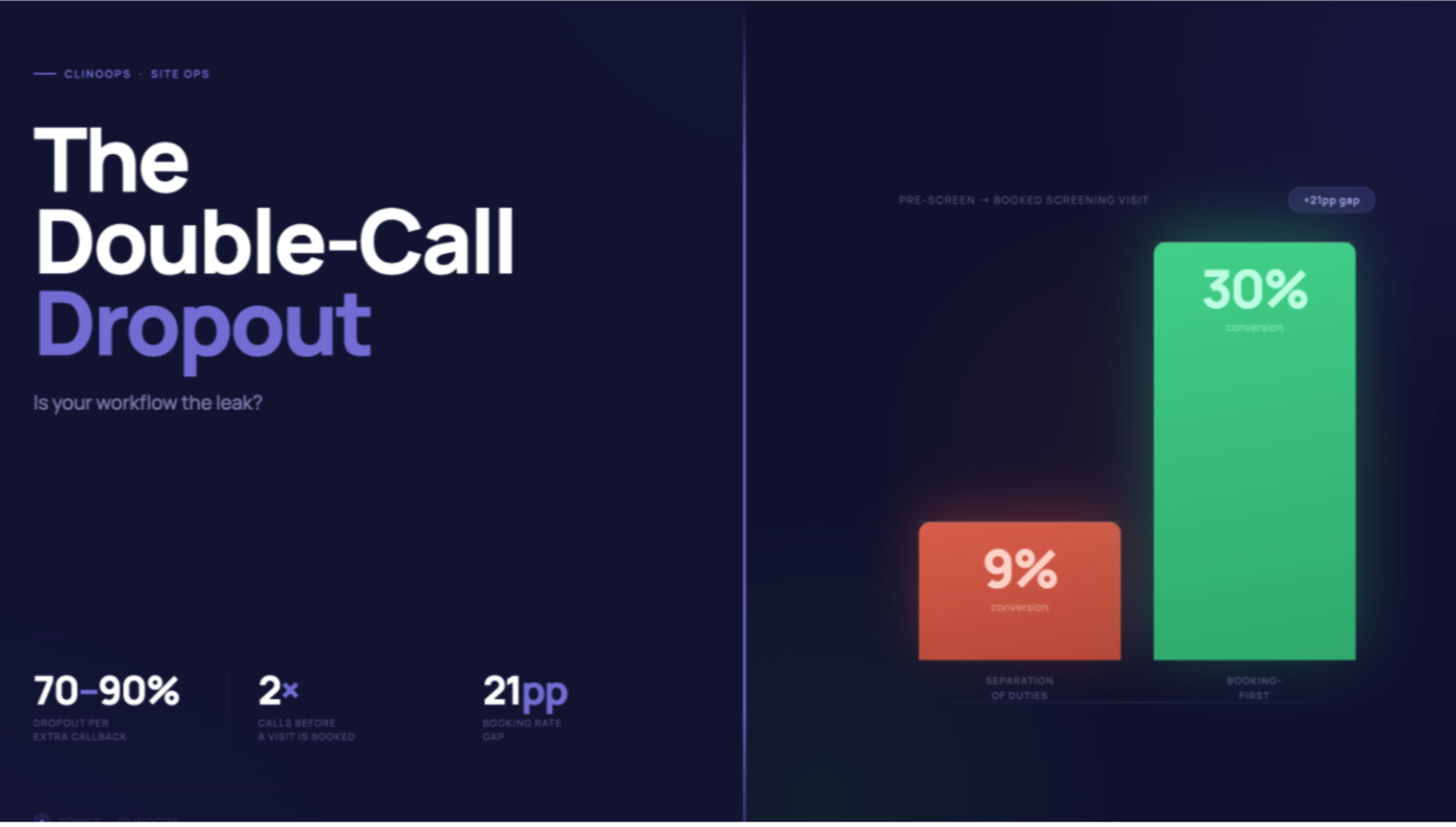
Because at larger sites, there's often a separation of duties between recruiters and CRCs. Recruiters handle the outreach, but can't confirm appointments. That's the CRC's job. So the patient sits in a holding pattern while a second call gets scheduled — at which point a CRC calls to... ask largely the same questions again.
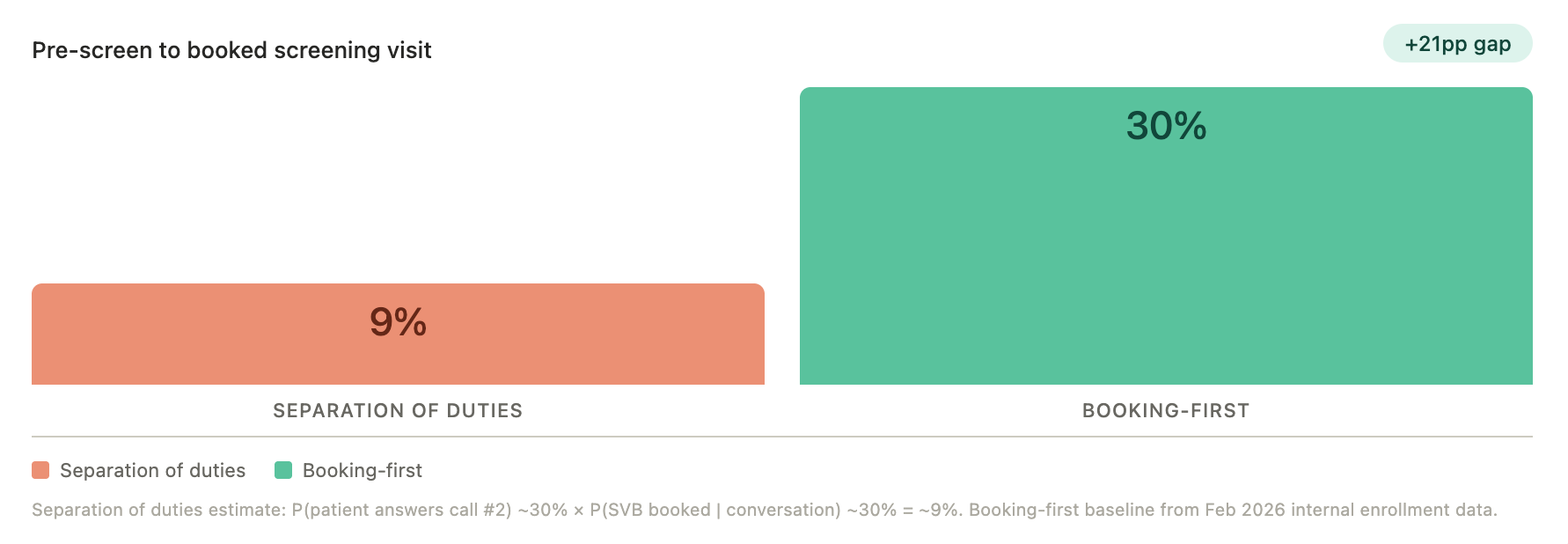
Each time you need to get a patient back on the phone, you're looking at a 70–90% drop in the funnel. That's not a rounding error. That's your pipeline.
That's the separation of duties problem. And in our experience working across dozens of sites, the ones running this two-step workflow tend to show materially worse full-funnel conversion rates than sites where the person doing the outreach can book directly.
"The momentum is important to the patient. Knowing that they have something on the calendar to look forward to is important versus having to wait for someone to call them to see if they qualify when they just spent 30 minutes on the line with the recruiter."
— David Ang, Head of Sites, Power
That's not a small thing. Patient motivation isn't static. It decays — and the principle applies here directly: every day between a patient's initial expression of interest and a confirmed appointment is attrition risk.
Why Sites Built It This Way
The rationale behind the separation of duties is understandable. There's a genuine concern that non-clinical staff — typically the recruiters doing outbound or inbound call volume — may lack the medical background to assess eligibility accurately. That's a fair concern.
But it's worth interrogating whether that concern holds up operationally, or whether it's been allowed to become an excuse for unnecessary friction.
When we've reviewed recruiter scripts and CRC scripts side by side across a number of our client studies, the degree of scientific complexity required at the pre-screening stage is frequently overstated. A well-designed eligibility script doesn't require clinical judgment so much as it requires thoroughness and structure. As David noted: "There's no rocket science here that someone couldn't at least do a good first pass on and collect the information that's relevant, even if they don't know all the scientific nuance behind it."
The nuance matters for edge cases. It rarely determines whether a patient should be offered a tentative screening appointment.
Two Ways to Fix It
There are two practical paths depending on your site's existing setup.
The first is script consolidation. Review what recruiters are asking versus what CRCs are asking. Where there's redundancy, eliminate it. Where there are CRC-specific questions, ask whether those can be moved upstream into the recruiter workflow. In most cases, they can be.
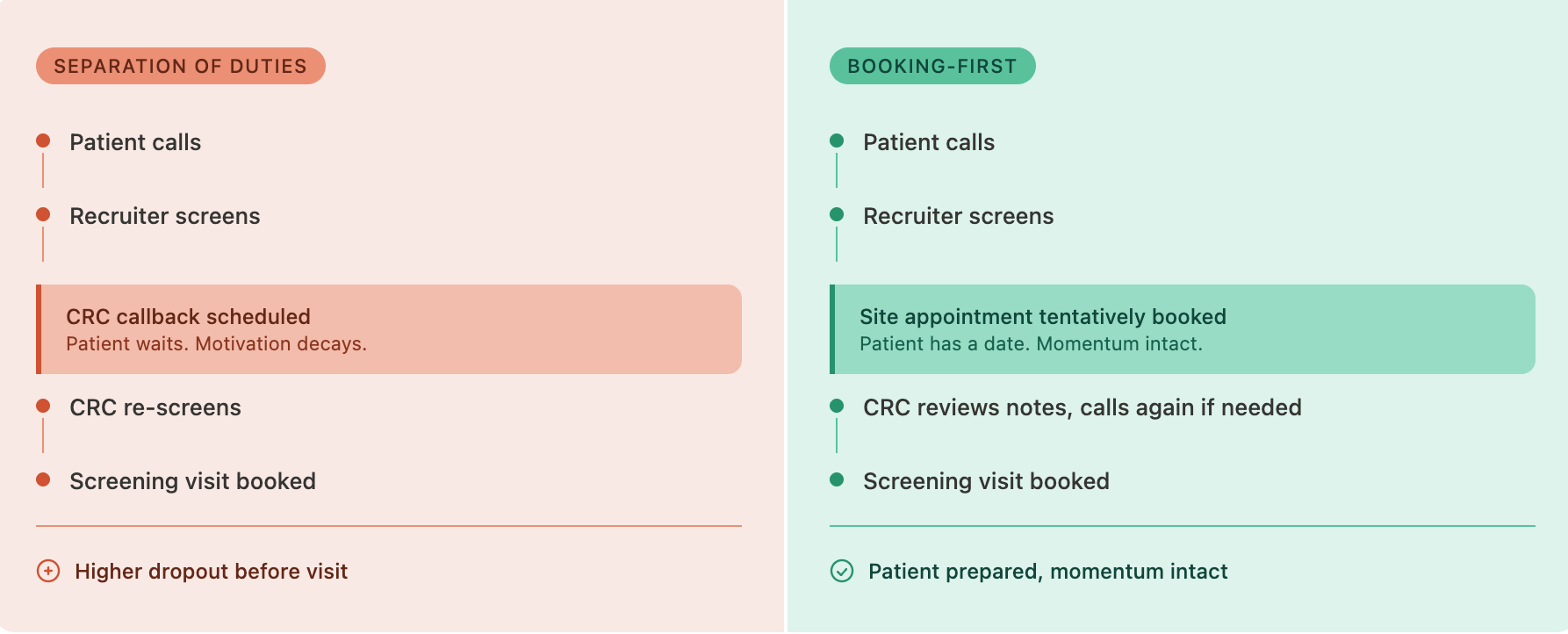
The second is a booking-first model, which is where the larger operational gain tends to be. Rather than making the booking contingent on a second clinical review, book the appointment tentatively at the end of the recruiter call. The patient has a confirmed date on their calendar. The CRC then uses the window between booking and visit to review the recruiter's notes, confirm eligibility, and call again if needed before the patient walks in the door.
Critically, this flips the psychological dynamic for the patient. They're no longer waiting to find out if they're "good enough" to be seen. They're already scheduled. The confirmation call from the CRC feels like preparation, not gatekeeping.
The Infrastructure That Makes This Work
For this model to hold up, the recruiter's intake process needs to produce structured, reliable documentation. Not freeform notes that get emailed over. Something the CRC can review quickly and consistently, knowing exactly where to look for the information they need.
This is something we've built directly into how Power's patient engagement team operates. The format is standardized across calls, so by the time a referral reaches a site, the CRC has a comprehensive intake summary that proactively answers the questions they'd otherwise need a second call to ask. Call recording and AI-assisted transcription can extend this further, with structured summaries generated automatically from recruiter conversations and reviewed before the follow-up call.
The Underlying Issue
Sites that convert at higher rates aren't typically working with better patient populations. More often, they've removed friction from a step that other sites treat as a necessary checkpoint.
The separation of duties workflow feels like quality control. In practice, it frequently functions as a dropout point.
If your site is running a two-call structure, it's worth asking one question: when was the last time you checked what percentage of patients who completed a recruiter call never made it to a CRC call? That number may be more informative than your screen-fail rate.
Power helps clinical trial sites and sponsors improve enrollment performance through better patient engagement infrastructure. Learn more at withpower.com